

Introduction: Poly (ADP-ribose) polymerase inhibitors (PARPi's) represent a newer class of antineoplastic agents targeting cancers with defective DNA-damage repair. PARPi's indications include subtypes of ovarian, fallopian tube and primary peritoneal cancer as well as subsets of patients with breast pancreatic and prostate cancers. There are currently 4 PARPi approved by the Food and Drug Administration (FDA): olaparib (approved 12/19/2014), rucaparib (approved 12/19/2016), niraparib (approved 3/27/2017), and talazoparib (approved 10/16/2018). The incidence of AML/MDS is known to be increased following chemotherapy, with a standardized incidence ratio (observed number of cases of AML/MDS among those treated with chemotherapy/expected number of cases in the general population) of 5.8 among patients with ovarian cancer, and 3.8 among patients with breast cancer (Morton et al, JAMA Onc 2018). All 4 PARPi also carry the potential risk of AML/MDS as an adverse event (AE), but a causal relationship has not been established. Notably, almost all patients treated with a PARPi would have exposure to cytotoxic chemotherapy prior to or during PARPi therapy. For patients treated with PARPi's in clinical trials, the duration of therapy prior to cases of AML/MDS emerging ranged from <1 month to 28 months. The incidence of AML/MDS observed in clinical trials with olaparib was <1.5%, rucaparib 1.1%, niraparib 0.8%, and talazoparib 0.3%. Real-world data regarding this rare but life-threatening AE in PARPi-treated patients is needed. We evaluated reports of AML/MDS associated with PARPi's in the post-approval setting.
Methods: The FDA Adverse Events Reporting System (FAERS) database was queried for AEs associated with any of the 4 approved PARPi's, from the date of the initial FDA approval for each agent (irrespective of the indication) through March 31, 2020. The FAERS database contains de-identified reports of product-related AEs, coded using the Medical Dictionary for Regulatory Activities (MedDRA) and classified as serious or non-serious. Cases reported outside the United States were excluded. The proportion of AML/MDS reports was analyzed overall and by PARPi. To account for the variation in length of time on the market due to the different approval dates, reports of AML/MDS for each PARPi were analyzed in the first 17 months after approval (the post-marketing period for the most recently approved agent). The indication for which the PARPi was used, the sex and age of the patient experiencing the AE, and the seriousness and outcome of the AE were assessed. Comparisons of the proportion of AML/MDS cases by agent were made using the Chi-square test; statistical significance was determined at a two-sided α=0.05.
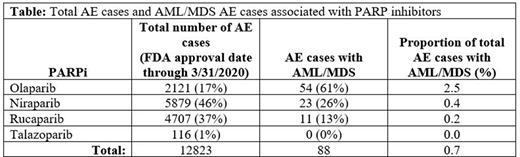
Results: A total of 12823 post-marketing AE reports were associated with PARPi's, with 88 (0.7%) reporting cases of AML/MDS (Table). The largest proportion of AML/MDS cases were associated with olaparib (54 of a total of 2121 AE reports; 2.5%, p<0.00001 vs. all other PARPi), followed by niraparib (23 of a total of 5879 AE reports; 0.4%) and rucaparib (11 of a total of 4707 AE reports; 0.2%). No AML/MDS cases were associated with talazoparib (0 of a total 116 AE reports). During the first 17 months following each agent's approval, 14 cases of AML/MDS were reported in association with olaparib, 10 with rucaparib, 9 with niraparib, and 0 with talazoparib. The majority of cases of AML/MDS occurred in women (73%), and the most common indication for treatment was ovarian cancer (52%). The median age of the patients in the AML/MDS reports was 66 years. Nearly all cases were classified as serious (98%), and the outcome of the AE was death for 28% of cases, hospitalization for 17% of cases.
Conclusions: Our retrospective analysis found that AML/MDS associated with PARPi's was reported rarely in the post-marketing setting, and that 60% involved olaparib. This study is limited by its retrospective design, and the possibility of under-reporting of cases to the FAERS database. Additionally, the time elapsed since approval differed by agent, and lower observed incidence of AML/MDS for some agents may reflect the limited duration of surveillance. No data is available in the case reports regarding length of exposure to chemotherapy. This real-world analysis complements existing clinical trial data and provides insight into AML/MDS associated with 4 different PARPi's in clinical practice.
Gajra:Cardinal Health: Current Employment. Zettler:Cardinal Health: Current Employment. Klink:Cardinal Health: Current Employment. Feinberg:Cardinal Health: Current Employment.

